
In July, 2013 the Insurance Research Council (IRC) published a compelling study entitled “Interstate Differences in Medical Utilization in Auto Injury Claims”. The study was based on a national sample of more than 20,000 BI liability claims and nearly 6,000 PIP claims closed with payment in 2012 from private passenger auto insurance companies that account for approximately 50 percent of the U.S. market1.
The study examined interstate variances in the use of common diagnostic procedures and treatments for claims where the most serious injury reported was a sprain or strain of the back or neck. These injury outcomes represented 59 percent of the BI outcomes in the study2. More specifically, the study looked at the frequency of use for each of the following: Magnetic resonance imaging, computed tomography, chiropractors and physical therapists (PT). The differences among tort states for chiropractor and PT treatments, which are the focus of this paper, are shown in Figure 13 below:
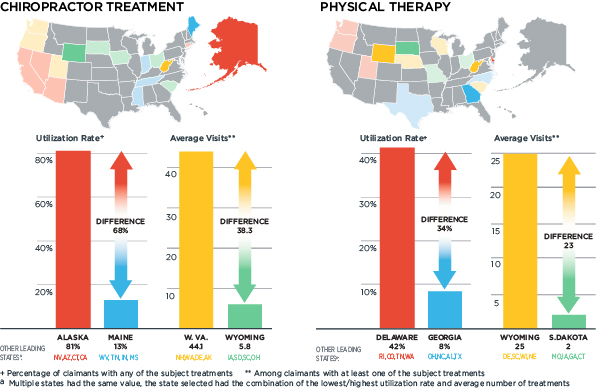
On the surface, as one examines variances in the frequency of the utilization and the average number of visits for these treatments by state, the expanse between the differences is disturbing. For those providers in the states with the lowest averages, are they simply more conservative in their use of treatments? Or, could they be that much more effective in discerning the need for treatment? And, when treatment is deemed necessary, are their treatments significantly more effective?
As for the states with the highest averages, what are the drivers of these behaviors? Do conditions in these states create an opportunity or need to cost shift? From an injury causation perspective, one would expect that states with more energetic collisions would tend to see more severe injuries and injury outcomes that require more treatment. The principle being that the higher the impact energy, the greater the potential for injury, and consequently, the greater the potential need for treatment. Could an explanation of the variances observed in the previously noted IRC study be that accidents in certain states are, in general, more or less severe in terms of the collision energy?
Let’s examine potential surrogate measures for collision energy in the tort states studied. Since airbags generally deploy in moderate to more severe auto collisions, a higher frequency of airbag deployments documented in total loss evaluations and vehicle repair estimates for the same year should indicate states where impact energy is, on average, higher. Additionally, a higher rate of traffic-related fatalities would also suggest higher average collision energy. Conversely, one might argue that the absence of fatal accidents or airbag deployments, as documented in total loss evaluations and vehicle repair estimates for the same year, would suggest a higher frequency of lower energy accidents, which would be consistent with injury outcomes where strains and sprains are the most severe injury reported.
Regression analyses among these variables showed some surprising results. On an individual basis, both fatality rates4 and the frequency of airbag deployments in liability auto physical damage claims5 in the states studied could explain a meaningful percentage of variance observed in the frequency of PT utilization. More specifically, as fatality rates and the rate of airbag deployments decrease, the average frequency of PT utilization increases. This observation is consistent with the hypothesis that the absence of fatal accidents or airbag deployments suggests that there is a higher frequency of lower energy accidents that would be consistent with injury outcomes where strains and sprains are the most severe injury reported.
Surprisingly, neither of these variables showed any significant ability to predict variance for the average frequency of chiropractic utilization or variances in the average number of visits made for PT or chiropractic treatment. In other words, variances in the average frequency of chiropractic utilization or the average number of visits made for PT or chiropractic treatment cannot be meaningfully explained by these surrogate measures of collision energy. This is troubling since it is well understood that collision energy is a proximate cause of auto injury and injury severity.
So, what can explain the significant discrepancies seen in the IRC findings? One possible explanation is that physicians and chiropractors are trained to take a history from the patient, conduct a physical and then relate the findings of the previous two steps into his/her diagnosis and treatment recommendations. These diagnoses and treatments rarely, if ever, include an objective and measured understanding of the collision energy experienced by the patient. The ultimate diagnosis and treatment is based on the healthcare provider’s perceived severity of the collision as described to him/her by the patient. Additionally, standards of care are also not linked to collision energy experienced by a patient. As a result of these circumstances, the opportunity for extreme variances observed in the IRC study exists.
Injuries are actually caused by a very specific physical stress or strain, or specific combinations of stresses and strains. In auto accidents, these requisite stresses and strains can be found to exist or not exist based on the amount of collision energy, position of the occupant in the vehicle use of restraint systems, and an analysis of the physics of the accident, among other factors. Additionally, when requisite stresses and strains exist, they also must exceed an individual’s tolerance, before the injury can be caused. And, the greater the requisite stresses and strains, the greater the potential for a more severe injury. As a result, the amount of energy in the accident should be considered to evaluate the severity of an injury, if it was indeed caused by the accident.
Scientific research regarding injuries produced by lower energy auto collisions (i.e., tests with impact related changes in velocity ≤ 10 mph) provides further insight into the variances documented in the IRC study. A meta-analysis of this research shows that well over 75 percent of the approximately 4,000 human subject test exposures produced no injury6. For tests that actually produced symptoms, over 60 percent of the test subjects noted symptoms for less than one day. The longest reported period of symptoms from a subject participating in a test with an actual impact was 14 days. Assuming three treatment days per week, a maximum number of expected visits would be six. It should be noted that this calculation is an estimate of the maximum visits, not the average number of visits previously noted in the IRC study.
Crash severity analytics show that an auto insurer can expect that roughly 50 percent or substantially more of the third party injury claims evaluated are associated with a low energy collision for at least one vehicle in the accident7. As a result, there is clear overlap in the frequency of collision events associated with outcomes documented in the referenced IRC study and the scientific research regarding injury outcomes in lower energy auto collisions. From a chiropractic care perspective, only the states found in the IRC study with very low frequency of utilization and very low average number of visits appear to have care outcomes that somewhat match with what is found in the previously noted scientific research. With respect to PT care, frequency of utilization appears to somewhat match with the same scientific research. However, the average number of visits matches only in those states with a very low average number of visits. These observations are consistent with the findings from the regression of the data in the IRC study with surrogate collision energy metrics.
When adjusting soft tissue injury claims resulting from auto accidents, how can the chaos and excesses highlighted by the IRC study be consistently avoided? What can be done to accurately assess the need for treatment and when needed, its duration?
Claim technologies exists today which calculate and characterize collision energy experienced by claimants from information in repair estimates and other metrics of vehicle damage. More precise measurements of collision energy can also be extracted from a vehicle’s event data recorder, commonly referred to as the “black box”. With collision energy data, claim technology can also evaluate the physics of an accident and its causal relationship to a claimed injury. Additionally, if the accident is capable of causing the claimed injury, the expected duration of symptoms can be assessed by comparing the injury to results observed at comparable energy levels in the previously-referenced human subject testing and scientific research.
As the data from the referenced IRC study suggests, periods of PT or chiropractic treatment may often exceed what is expected from a low energy accident capable of producing a strain. In these cases, a review of medical bills can complement a scientific evaluation of injury causation and symptom duration. Medical bill reviews, which can also be technology based, highlight irregularities in invoices for medical care, including inappropriate treatments for the diagnoses, unusual pricing for procedures, and delays or gaps in treatment. When irregularities identified from a medical bill review are significant and treatment duration exceeds the expected duration of treatment from a scientific evaluation, questionable treatment and related costs can be more comprehensively and confidently addressed.
Integrated technology platforms that offer both scientific causation analytics from vehicle repair/damage data and comprehensive medical bill review analytics will soon be available to facilitate a more seamless and comprehensive evaluation of injury claims. The result promises a more objective, efficient and effective way to consistently and accurately evaluate injuries. Or, in other words, provide valuable assistance to claims organizations working to appropriately diminish the significant expanse in outcomes for both the utilization and duration of certain treatments.
*******
1 – Insurance Research Council, “Interstate Differences in Medical Utilization in Auto Injury Claims”, 2013, page 9.2 – Ibid, page 5.
3 – Ibid, pages 31, 35.
4 – U.S. Department of Transportation Fatal Accident Reporting System, 2012.
5 – CCC Intelligent Solutions
6 – CCC Intelligent Solutions
7 – CCC Intelligent Solutions